View the up-to-date information for the 2026 Annual Meeting.

Press Release
Contact
Molly McDougall/
Jeanne-Marie Phillips
HealthFlash Marketing
203-977-3333
molly@healthflashmarketing.com
Sharon Grutman
The American Society of Breast Surgeons
877-992-5470
sgrutman@breastsurgeons.org
Download
Lumpectomy as Effective as Mastectomy for Young Breast Cancer Patients
New Study Finds More Extensive Surgery Does Not Affect Survival
- Abstract: Young Women with Breast Cancer: Does Surgical Approach Impact Overall Survival?
Las Vegas, April 6, 2022—Young women with breast cancer experience similar survival whether treated with mastectomy (full breast removal) or lumpectomy (removal of a tumor with a surrounding margin of healthy tissue), despite tumors that are typically more aggressive and discovered at a later stage compared to their older counterparts. These were the findings of a new study examining women with non-metastatic breast cancer under age 40 presented this week at the American Society of Breast Surgeons annual meeting. The study is among the largest on the impact of surgical approach on survival outcomes in a young patient population.
“The results are particularly significant because younger women are increasingly being diagnosed with breast cancer, despite low rates overall, and a growing number are undergoing mastectomy and even prophylactic bilateral mastectomy rather than breast conserving surgery,” says Christine Pestana, MD, Breast Surgical Oncology fellow at Atrium Health, Levine Cancer Institute, and lead study author. “Studies like this show that lumpectomy, a far less aggressive approach with fewer potential complications and morbidity, is equally as effective as removing an entire breast.”
Dr. Pestana believes that many young women may be influenced by their age and equate an aggressive approach with better long term survival. However, with mastectomy comes greater risk of problems such as infection, wound issues, chronic pain and subsequent multiple reconstructive procedures. “A decision on breast cancer surgical treatment has many implications, and these women will live with them the rest of their lives,” she says, noting that younger women with breast cancer may constitute a unique and under-represented population. “Studies specifically focusing on these patients would likely yield important information that may help physicians better understand, counsel and treat these patients and help women in their decision-making.”
The retrospective study examined 591 patients in the Young Women’s Database at Levine Cancer Institute who were diagnosed with cancer and treated surgically between 2010 and 2018. Patients were stratified based on hormone receptor (HR) and HER2 status. Along with type of surgery, demographic data and information on stage, tumor grade, and the use of hormone and systemic therapy were collected. The mean patient age was 37, and women were followed up to 67 months post-surgery. The mortality across all groups was 12%.
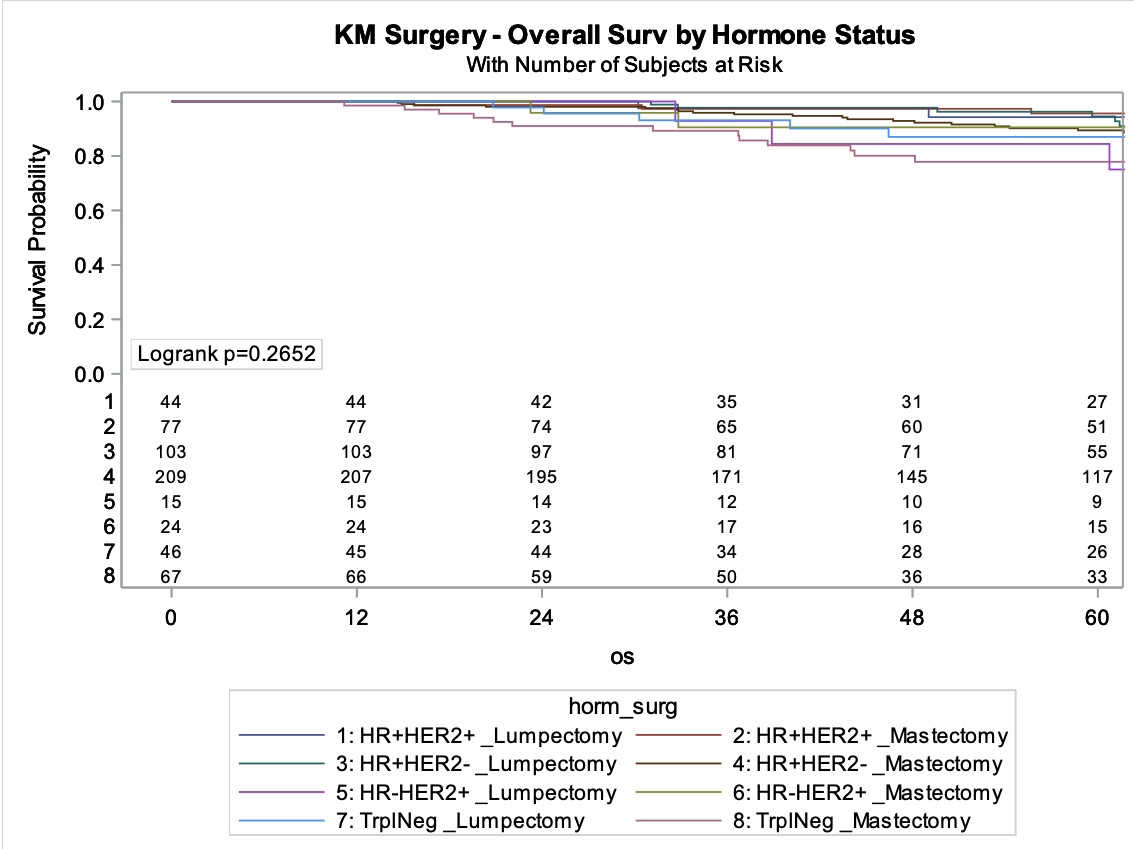
Overall, treatment with mastectomy versus lumpectomy had no impact on survival. Additionally, survival was similar across HR and HER2 subtypes. However, within the HR+/HER2- group, failure to comply with hormonal therapy when it was prescribed was associated with a higher risk of death. Black patients with triple negative cancers also had higher mortality. No other factors examined were associated with lower survival.
Dr. Pestana notes that younger patients have historically been excluded from breast cancer studies, yet the diagnostic and treatment frameworks that emerge from this research are applied to them. Additionally, studies show that many women have family histories and other breast cancer risk factors that were not identified prior to diagnosis. Often, these factors flag patients for discussion of cancer surveillance, preventative therapy and can potentially lead to an earlier diagnosis.
“Breast cancer is a particularly difficult disease for younger women. The medical system should prioritize empowering cancer patients and those at risk with research, guidance and information focusing on their specific age group,” she notes. “Patients may benefit from consulting with several doctors to take advantage of multiple perspectives. Peace-of-mind is an important consideration. Ultimately, patients must be comfortable with their decision, and their doctors should support an informed choice.”
Abstract, Official Proceedings
Young Women with Breast Cancer: Does Surgical Approach Impact Overall Survival?
Authors: Christine Pestana1, Sally Trufan2, Courtney Schepel2, Terry Sarantou2, Richard White2, Lejla Hadzikadic-Gusic2
Institutions: 1Atrium Health, Levine Cancer Institute, Winston Salem, NC, 2Atrium Health, Charlotte, NCObjective: Young women with breast cancer can often present with advanced disease when compared to their older counterparts. Outcome disparities persist between the two groups. Mastectomy rates are increasing in younger patients despite lack of data supporting improved survival. This study investigates the association between surgical approach and survival in young patients with breast cancer.
Methods: We performed a retrospective chart review of 885 women < 40 years old included in the Young Women’s Database at a single institution. 294 subjects were excluded due to missing data. 591 subjects with non-metastatic invasive breast cancer between 2010 and 2019 who received surgical intervention were included in the analysis. Details regarding patient demographics, tumor characteristics, molecular subtype, and treatment were collected. Patients were stratified based upon molecular subtype, and descriptive statistics were performed. Univariable and multivariable Cox proportional hazard analyses were performed to determine if patient, disease, or treatment factors were associated with an increased risk of death. Significance was set at p <0.05.
Results: The median age for the cohort was 37 years (IQR 34-39) and time to follow up was 67 months (IQR 41-98). Overall, 12% of patients died (N=72). Molecular subtypes included: HR+/HER2- (n=315, 53.3%), HR+/HER2+ (n=123, 20.8%), triple negative (n=114, 19.3%), and HR-/HER2+ (n=39, 6.6%). Variables assessed for association with overall survival included age, race, BMI, disease stage, grade, presence of lymphovascular space-invasion, extranodal extension, extent of surgery (breast conservation vs mastectomy), presence and timing of chemotherapy (neoadjuvant, adjuvant, none), and presence of hormonal therapy (when appropriate). 85.4% of the HR+/HER2- group took antiestrogen therapy. On multivariable analyses in this group, only an absence of hormone therapy was significant, with a 2.9 increased risk of death for patients who did not take hormone therapy when compared to those using it (p=0.02). On univariate analysis, black race was associated with an increased risk of death in all molecular subtype categories. However, on multivariate analysis, this only held true in the triple negative group, where black race was associated with a 5.7 times increased risk of death (p=0.005) even after accounting for all other risk factors. No associations of note were seen for the HR+/HER2+ or HR-/HER2+ groups. The use of mastectomy versus breast conservation did not impact overall survival in any of the molecular subtypes.
Conclusions: Overall survival does not differ based upon type of surgery in younger patients with breast cancer. Counseling regarding outcomes is important, especially in reducing unnecessary morbidity from surgical procedures that are not indicated given the increased use of mastectomy in this age group.