View the up-to-date information for the 2026 Annual Meeting.

Press Release
Contact
Molly McDougall/
Jeanne-Marie Phillips
HealthFlash Marketing
203-977-3333
molly@healthflashmarketing.com
Sharon Grutman
The American Society of Breast Surgeons
877-992-5470
sgrutman@breastsurgeons.org
Download
COVID-19 Significantly Delayed Breast Cancer Care at Safety-Net Hospital
New Study Tracks Treatment Patterns of Vulnerable Patients
- Abstract: Impact of COVID-19 Restrictions on Stage of Breast Cancer at Presentation and Time to Treatment and Surgery at an Urban Safety-net Hospital
Las Vegas, April 6, 2022—One-year local COVID-19 restrictions negatively impacted breast cancer stage at presentation, time to treatment and time to surgery at an urban safety-net hospital, increasing the vulnerability of an already high-risk population. These were the findings of a new study presented at the American Society of Breast Surgeons annual meeting, which compared breast cancer care before and after COVID restrictions.
“We hypothesized that the pandemic would cause delays across all parameters studied, and our research corroborates this,” says Kelly Kapp, MD, PGY-4 General Surgery Resident at University of Missouri-Kansas City School of Medicine and lead study author. “Given that our population already had a history of presenting with three-fold higher rates of late stage cancer pre-pandemic, the increased risk and the implications for care and outcomes are enormous.”
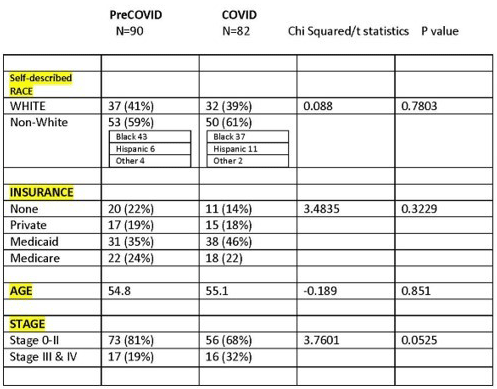
In the IRB-approved study, 82 patients diagnosed with breast cancer from March 2020 to April 2021 were identified through the institution’s breast cancer registry. They were compared with 90 similar patients included in the same database from March 2018 to February 2019. Data was collected on all parameters being studied as well as on patient demographics. Late stage cancer was defined as stage III or IV.
After controlling for race and type of insurance coverage, women were 1.2 times more likely to present with late stage disease during COVID restrictions than prior to COVID. Mean time to first treatment was 48 days compared to 29 days pre-COVID. Mean time to surgery, when it was the first treatment, was 65 days during COVID and 36 days pre-COVID.
“These delays were likely caused by a range of factors,” says Dr. Kapp. “Safety-net hospital populations generally have less access to childcare and transportation. Often they do not have the type of employment that offers remote work options, making their schedules less flexible. The pandemic may have exacerbated these issues. We also know this population became more disenfranchised during COVID.”
Dr. Kapp believes that proactive outreach is important to help safeguard the health of safety-net populations. Public service announcements, communications through primary care physicians and telephone reminders all might help re-engage women in their healthcare.
“A pandemic and other ongoing situations that affect access to care can happen again,” Dr. Kapp comments. “Patients at safety-net hospitals already are significantly disadvantaged and COVID set them back even more. We must make sure that this does not happen again.”
Abstract, Official Proceedings
Impact of COVID-19 Restrictions on Stage of Breast Cancer at Presentation and Time to Treatment and Surgery at an Urban Safety-net Hospital.
Authors: Kelly Kapp, An-Lin Cheng, Nasim Ahmadiyeh
Institution: University of Missouri - Kansas City School of Medicine, Kansas City, MO
Objective: The COVID-19 pandemic disrupted health systems, with the Center for Disease Control recommending postponement of elective surgeries and medical procedures in March 2020. While cancer surgeries continued, screening mammograms declined during this time and clinics were disrupted. Even pre-pandemic, patients accessing our urban safety-net hospital presented with three-fold higher rates of late-stage breast cancer than other Commission on Cancer (CoC) accredited sites across the country. Here we sought to determine the effect, if any, of the COVID pandemic on stage of breast cancer presentation, time to first treatment and time to surgery at an urban safety-net hospital. We hypothesized that the pandemic would be associated with an increase in late-stage breast cancers at diagnosis among an already vulnerable safety-net population and expected to see delays in care.
Methods: An IRB-approved cohort study was conducted at an urban safety-net hospital. The COVID cohort spanned March 2020 when the local “stay at home” order was issued through February 2021 when restrictions were lifted. This was compared to a pre-COVID control cohort from March 2018-February 2019. Patients with new breast cancer diagnoses (172, 90 pre-COVID, 82 during COVID) were identified through institutional Cancer Registry. Stage at presentation, time to first treatment, time to surgery as well as demographic information including race and payer were collected and compared between the two cohorts using multivariate logistic regression, SAS. Late-stage disease was defined as Stage III or IV following AJCC 8th edition.
Results: Both cohorts had similar baseline characteristics (Table 1). Patients were more likely to present with late-stage disease in the COVID Cohort than pre-COVID (31.7% vs 18.9% p=0.05). Multiple logistic regression controlling for race and insurance showed that it is 1.2 times more likely for our safety-net women to present with late-stage disease during COVID restrictions as compared to pre-COVID (p<0.05). There was longer time to first treatment and longer time to surgery (when surgery was the first treatment) during COVID than pre-COVID (median 48 days vs 29 days to first treatment; median 65 days vs 36 days to surgery; both p<0.001).
Conclusions: Even before the pandemic, women accessing our safety-net were significantly more likely than women at other CoC sites across the country to present with late-stage breast cancer. Here we have shown that the pandemic further exacerbated this problem among our safety-net women, making it significantly more likely that they presented with late-stage breast cancer during COVID restrictions than before. We also showed a longer time to first treatment including time to surgery during COVID. Reasons for this are likely multifactorial. Institutional factors alone do not account for the delay since clinics were only briefly closed and cancer surgeries never stopped (though screening mammograms did). There may have been a perception on the part of patients that care was not accessible during this time, and stressors and competing priorities may have contributed to delays in seeking care. Every effort should be made to minimize disruption to safety-net hospitals during future shut-downs or public health crises, as these patients are already among our most vulnerable.